
Many thanks to Dr. David Migneault (Emergency Medicine physician and Ethicist at Vancouver Coastal Health) for a really insightful, thought-provoking, and engaging noon rounds on the topic of navigating Requests for Non-Beneficial Care. He covered core ethical tenets as well as cases that are commonly seen on the medicine wards.
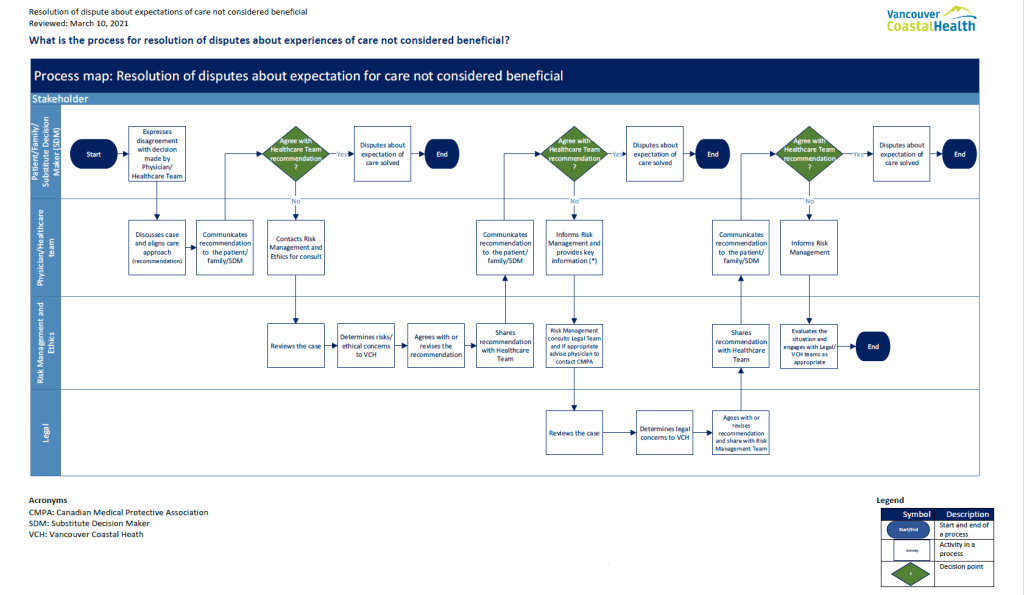
Please see below a process map for Resolution of disputes about expectation for care not considered beneficial.
Key takeaways:
Non-Beneficial Care – Futility
- This is the deliberative clinical judgment that clinical management is no longer reliably expected to
achieve its outcome. - To be clinically useful, judgments of futility
must be specified as either physiologic futility, imminent demise futility, clinical or overall futility, or quality of life futility.- Physiology futility: clinical judgement that clinical management is no longer reliably expected to result in its intended (and clearly specified) outcome.
- Imminent demise futility: clinical judgment that continued life-sustaining treatment will be physiologically effective for a short time, but that the patient is expected to die in the foreseeable future and not recover any interactive capacity beforehand.
- Quality of life futility: clinical judgment that life-sustaining treatment is physiologically effective, will
prevent imminent demise, and will preserve interactive capacity but will result in a quality of
life that is unacceptable to the patient.




Leave a comment