We reviewed a case of a post-renal transplant patient presenting with diffuse pustular skin lesions, unresolving pneumonia with parapneumonic effusion, and multiple brain lesions due to disseminated Nocardia.
Here are the didactic slides from our noon report
A few summary points:
- Transplant ID is a really complex field and you aren’t going to master this on your own – lean on our expert consultants. For our purposes it is important to recognize that infectious sources in the post-transplant setting include:
- The infections anyone can get (CAP, UTI, cellulitis, etc)
- Weird and wonderful infections due to immunosuppression
- Donor derived infections
- Multi-resistant organisms picked up through extensive hospital contact immediately peri-transplant.
- Timeline matters
- <1 month post-transplant: Think about hospital-acquired infections, line infections, C diff, pre-existing infections. Shouldn’t expect opportunistic infections yet!
- 1 month-6 months: Start thinking about opportunistic infections as often immunosuppression is high in this periods, especially note if there has been interruption in antimicrobial prophylaxis eg Septra
- >6 months: If immunosuppression dose lowered, returns to ~community-acquired sorts of infections. If immunosuppression remains high (eg to maintain adequate function in dysfunctional allografts), remain at high risk for opportunistic infections.
- Septra is really important prophylaxis for periods of deep immunosuppression – prophylaxis against PJP (we know), but also Nocardia, Listeria and Legionella!
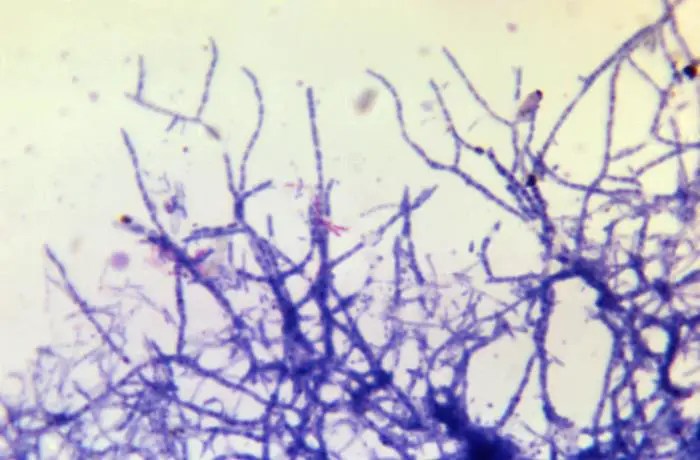
- To briefly summarize Nocardia, the illness script would be in an immunocompromised patient presenting with pneumonia (usually) +/- skin/brain involvement in disseminated disease. SEPTRA is the backbone of treatment (different regimens for different presentations and severity), generally for at least 6-12 months duration. Transplant ID should be making these decisions with you.
AM – This is my last noon report as your chief resident! It’s been a pleasure deep diving into these cases and having the opportunity to teach you about some wild IM presentations, and hopefully a few things you can use in your future practice!! Have a wonderful holiday and I’ll see you on the wards 🙂




Leave a comment