Slides from today’s noon report
Fever of unknown origin NEJM review 2022
Teaching pearls
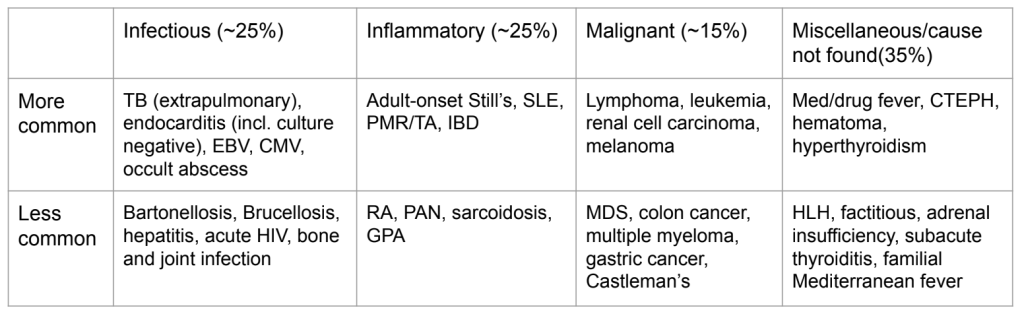
Consider a wide differential including infectious (25%), inflammatory (25%), malignant (15%), misc (35%) etiologies
FUO workup is done in tiers
- First tier
- Thorough history and physical
- CBC, CRP, ferritin, TSH, RF, ANA, HIV/Hep serology, blood cultures x 3 +/- EBV/monospot/Q-fever serology
- Urinalysis and culture
- TB skin test or IGRA
- CT chest abdo pelvis
- TTE
- Second tier
- Repeat thorough history and physical
- Discontinue non-essential medications (esp those associated with drug fever)
- Leg Doppler for DVT
- 18-FDG PET/CT scan vs WBC scan
- Third tier
- Repeat thorough history and physical
- Chase any findings with investigations
- Consideration of empiric use of NSAIDs, steroids
Intravascular lymphoma
- Rare subtype of large cell lymphoma in which malignant cells (CD20 expressing) proliferate within the lumina of small blood vessels – no circulating lymphoma cells in peripheral blood (90-95% cases), no obvious extravascular tumor mass
- Quite rare – annual incidence <0.5 cases per 1,000,000. Usually affects elderly (avg age at diagnosis approx 70), M = F
- Highly variable presentation:
- Pain, organ-specific local symptoms, multiorgan failure, FUO
- >50% have systemic symptoms (fever, B symptoms)
- Cutaneous involvement in 40% (heterogenous range of lesions, commonly in the chest/lower abdomen/extremities)
- Highly variable neurological involvement in 35%
- Diagnosed by biopsy – skin lesion if present, or affected organ. If there is no clear focus, random skin biopsies described in the literature.
- Treated by chemotherapy (eg R-CHOP)
- Limited data around prognosis, although a case series (n=10, single institution in Taiwan) showed improved survival in those who were caught in time and completed chemotherapy.




Leave a comment