Thanks for joining us!
Here are the presentation slides for our review of EMPA-KIDNEY
Credit to NephJC/Freely Filtered Podcast/ACP Journal Club who I borrowed some insights from for this discussion. Thanks to Dr. Claire Harris of Nephrology for her input as well.
Key takeaways:
This study extends evidence for renoprotection with SGLT2i to non-diabetic patients and those with eGFR 20-30. More pronounced benefits in those with higher levels of proteinuria and patients with diabetes.
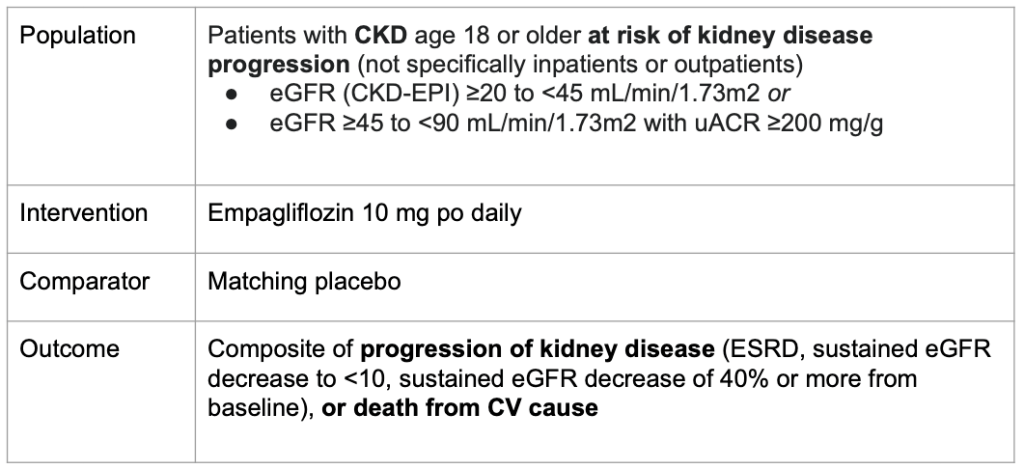
- Large sample size (n=6609) across 241 centres in Europe, North America and East Asia capturing CKD patients with high risk of kidney disease progression. Specific focus on inclusion of non-diabetic patients and those with lower levels of albuminuria (limitations of CREDENCE and DAPA-CKD).
- Composite primary outcome of kidney disease progression or cardiovascular death occurred in 432/3304 (13.1%) patients in the empagliflozin group vs 558/3305 (16.9%) patients in the placebo group (HR = 0.72, 95% CI 0.64-0.82, P<0.001)
- Effect preserved in non-diabetics, down to eGFRs under 30, but with less convincing effect with lower albuminuria
- Empagliflozin associated with initial GFR drop (related to release of tubuloglomerular feedback -> afferent arteriolar vasodilation -> reduction in intraglomerular pressure, decreased GFR) with improved GFR decline slope subsequently (less hyperfiltration)
- CV mortality not an impressive outcome in this study, maybe unsurprising as only ~25% of this sample had CV disease history.
- Good safety profile – do need to counsel patients around urinary tract infections. Very small rates of ketoacidosis.
- Low albuminuria group difficult to sort out as the trial was stopped early for efficacy, and these patients have lower baseline rate of renal function decline – it will be more difficult to confidently show improvements in progression of kidney disease without a longer trial.




Leave a comment