
Here are the slides for today’s presentation on cirrhosis
Key Takeaways:
- On consults, communicate whether cirrhosis is decompensated vs compensated, grade severity with Child Pugh C or MELD (MELD-Na), include the underlying etiology if known.
- Remember the key “sub issues” under cirrhosis management: Etiology, varices, ascites/SBP, hepatic encephalopathy, HCC, prevention, follow-up
- Commit to memory your approach to massive variceal bleeding
- ABC MOVIE, large bore IVs, head of the bed 90 degrees (aspiration risk), stat labs, cross matching for 3+ units of blood and plan to give FFP as well, phone calls to ICU and GI immediately, panto/octreoxide/ceftriaxone
- Everyone with new ascites needs a diagnostic paracentesis (SAAG calculation, culture, cytology)
- Salt restriction indicated for ascites, fluid restriction only if concurrent hyponatremia
Updates in 2023!!! (Dec 5, 2023)
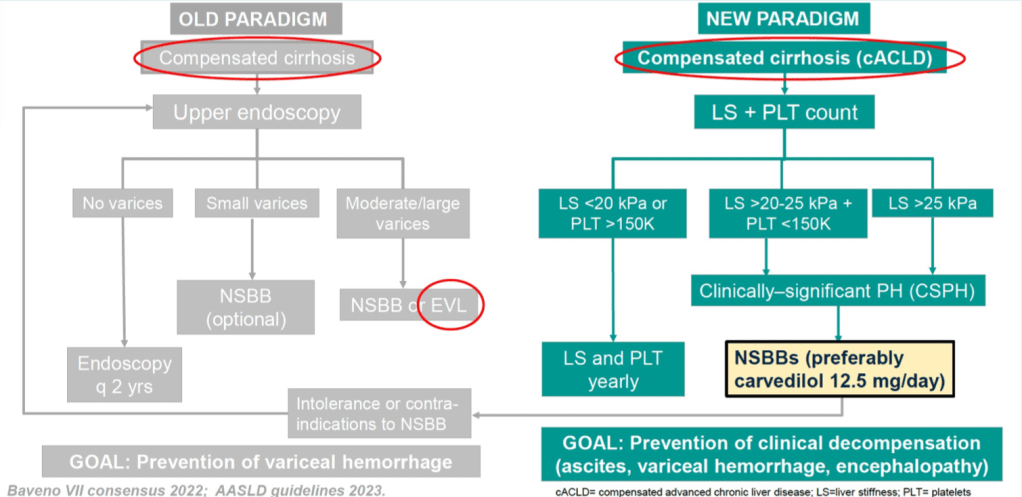
- Carvedilol is the preferred beta-blocker for variceal bleed ppx
- AASLD 2023: HCC screening by ultrasound and serum AFP q6months (sensitivity of US alone 53%, but US+AFP sensitivity 63%).
- Recommendation not yet adopted by CASL (no new Canadian guidelines since 2018)
- EGD no longer uniformly recommended for variceal screening in new diagnosis of compensated cirrhosis (risk stratification with liver stiffness by Fibroscan + PLT count -> carvedilol if high risk; scope only if intolerant/CI to beta-blocker)




Leave a comment