Thanks Dr. Galm for an excellent session on prolactinomas and the other etiologies of elevated prolactin
Key takeaways
- Clinical exam should include:
- Direct effects of prolactin – hypogonadism (oligo/amenorrhea, low testosterone, bone loss) and galactorrhea
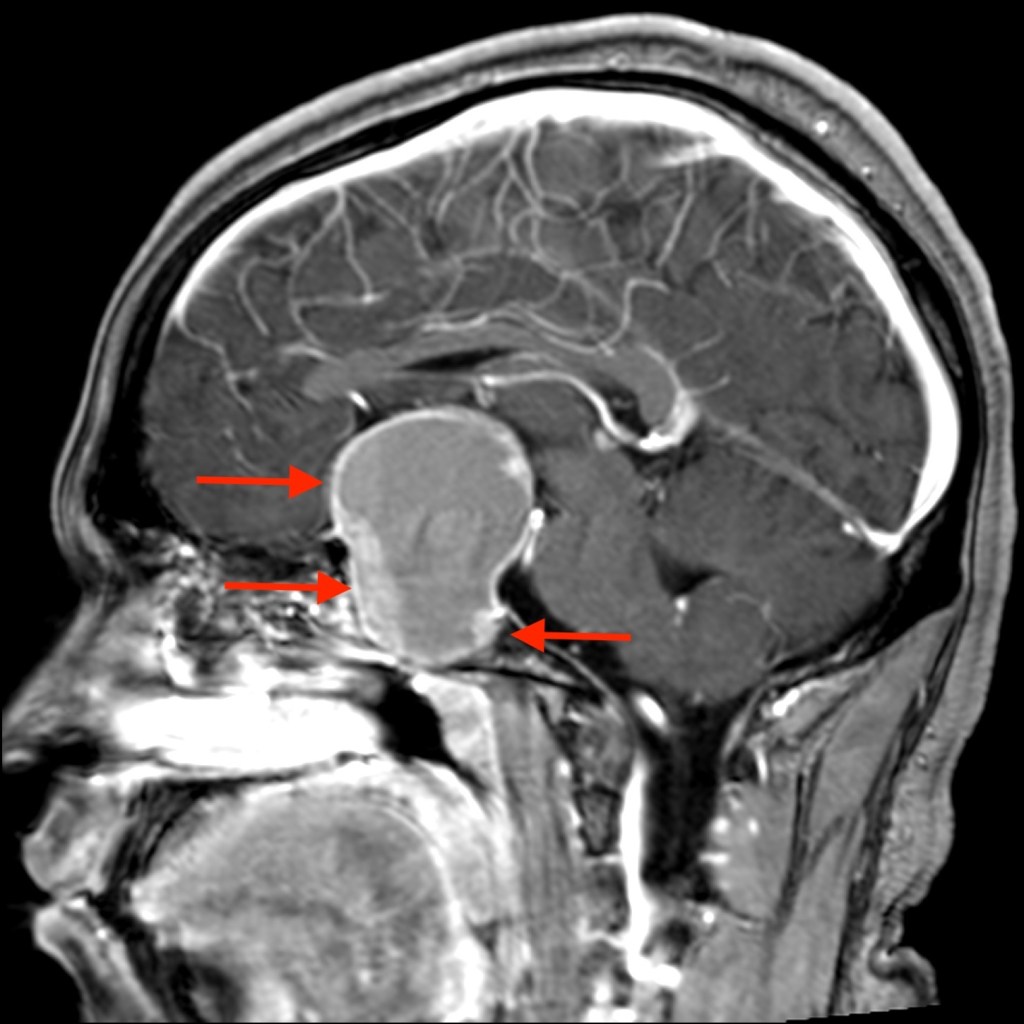
- Evidence of mass effect (HA, bitemporal hemianopsia, other symptoms and signs of hypopituitarism)
- Differential including:
- Physiologic (pregnancy/lactation, stimulation/illness/stress, eating)
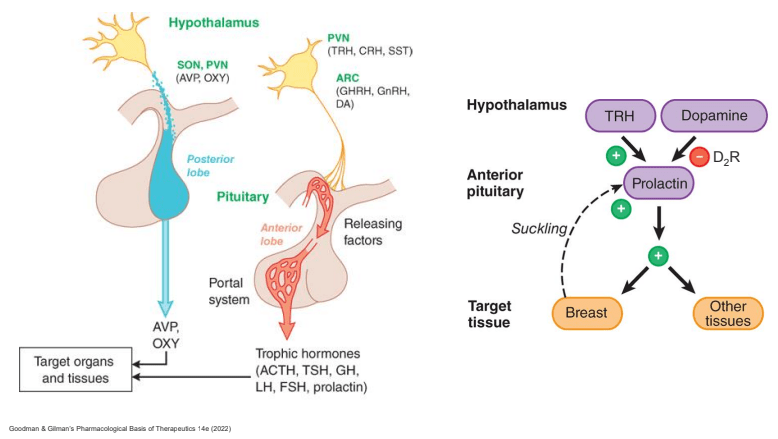
Medications (anti-psychotics, antiemetics, opioids, estrogen) - Pituitary disease (prolactinoma, stalk effect, acromegaly** (co-secretion of IGF-1 and PRL))
- Misc causes
- Look out for stalk effect, macroprolactin (up to ~9% high PRL), hook effect
- Physiologic (pregnancy/lactation, stimulation/illness/stress, eating)
- Most common cause is prolactinoma (micro > macro), followed by drug-induced
- If high PRL caused by prolactinoma, expect PRL ~100 for prolactinoma 1 cm. PRL over 500 is always due to prolactinoma
- Management
- Cabergoline preferred to bromocriptine (efficacy, less side effects, less frequent dosing)
- Review list of key adverse effects to counsel patients around
- Important distinction with respect to surgical vs medical management is whether high PRL is due to STALK EFFECT (needs surgery) vs PROLACTINOMA (needs dopamine agonist up front, even when large and with visual symptoms)
- Cabergoline preferred to bromocriptine (efficacy, less side effects, less frequent dosing)




Leave a comment